

The 2022 KFF Women’s Health Survey found that one-third (33%) of female hormonal contraceptive users have missed taking their birth control because they were not able to get their next supply on time. Furthermore, it is estimated that more than 19 million women of reproductive age in need of publicly-funded contraception live in an area considered to be a contraceptive desert, meaning there is limited access to a publicly-funded provider who offers contraception. Research also points to the impacts of state and federal policies on the shrinking number of family planning providers that offer the full scope of contraceptive methods in some communities.
In recent years, there has been public discussion and state and federal policy action to reduce contraceptive access barriers by expanding the availability of daily oral contraceptive pills through different mechanisms. Approaches that have been adopted include making OCP available over the counter without a prescription; expanding the ability of pharmacists to dispense or prescribe OCP; extending the supply of contraception that is dispensed at one time; and using mail-based online services or smartphone applications.
Over the Counter (OTC) Access
In July 2023, the U.S. Food and Drug Administration (FDA) approved the progestin-only Opill for OTC use, making it the first OTC daily oral contraceptive pill. Opill is available for over-the-counter purchase without age restriction in stores and online. The suggested retail price of Opill is $19.99 for one month’s supply or $49.99 for three month’s supply. Although it is farther behind in the process, another pharmaceutical company, Cadence, is working toward FDA approval of an OTC version of its combined (progestin and estrogen) oral contraceptive pill, Zena.
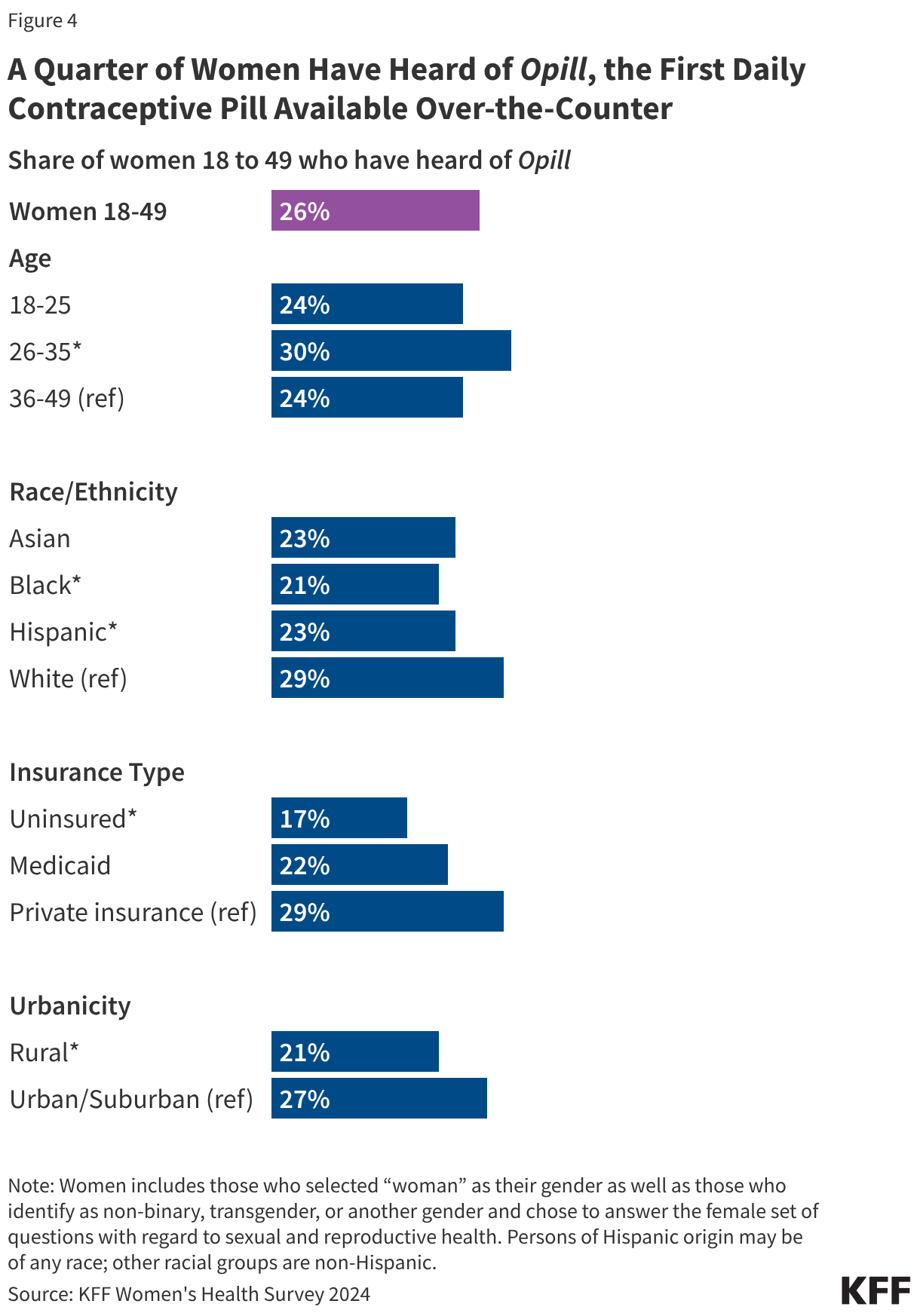
Research suggests that OTC access would increase the use of contraception and facilitate continuity of use. It could also allow women to save time spent on travel, at doctor’s office, and off work. Other research suggest that OTC oral contraceptives can especially benefit populations who have historically faced barriers to accessing contraceptive care, such as young adults and adolescents, those who are uninsured, and those living in contraceptive deserts or areas with limited access to health centers offering the full range of contraceptive methods. However, just a quarter (26%) of women 18 to 49 saying they have heard of the new daily oral contraceptive pill, and smaller shares of women who are uninsured (17%) and who live in rural areas (21%) have heard of Opill compared to those with private insurance (29%) and those living in urban or suburban areas (27%) (Figure 4).
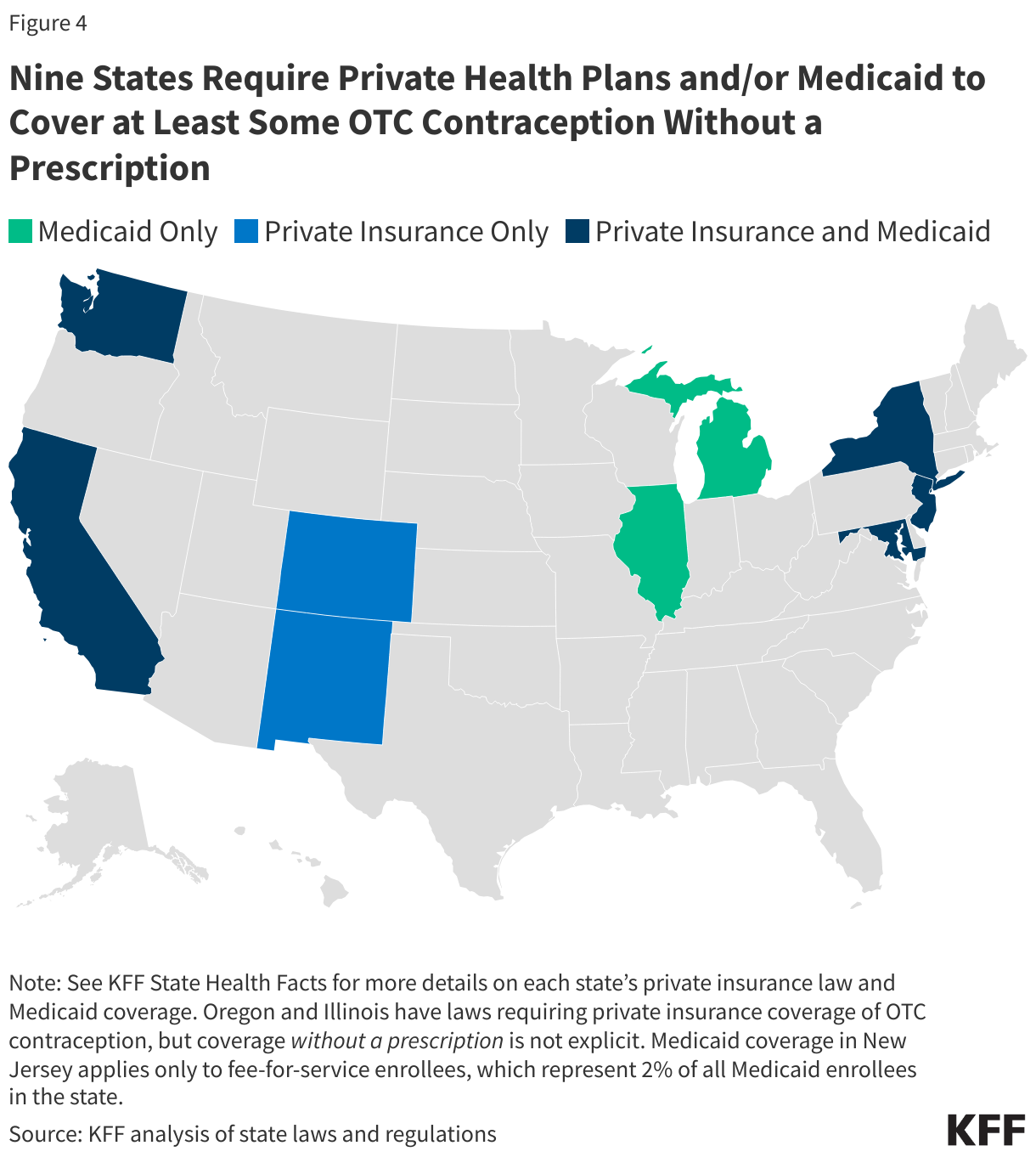
The ACA currently requires no-cost coverage for contraceptives in most private plans and for Medicaid expansion populations but plans typically require a prescription in order to trigger coverage, even for contraceptive methods that are available OTC without a prescription. Requiring plans to cover non-prescribed contraceptives would require legislation at the federal or state level, or administrative changes to the ACA’s preventive services policy. Nine states (CA, CO, DE, MD, ME, NJ, NM, NY, and WA) have laws or regulations requiring state-regulated private health insurance plans (individual, small group, and large group markets) to cover, without cost sharing, OTC contraception without a prescription. While New York’s law applies to emergency contraception only, the other state laws apply to non-prescribed contraceptive drugs broadly(Figure 5).
Eight states (CA, IL, MD, MI, NC, NJ, NY, and WA) use state-only funds to cover at least some OTC contraception without a prescription for Medicaid enrollees. However, these states, with the exception of California, cover non-prescribed emergency contraception and/or condoms only, so a change in law or policy would be needed to cover a daily oral contraceptive pill without a prescription. States wishing to cover OTC contraception without a prescription for enrollees must use state-only funds as federal funds are only available for prescribed drugs. (See KFF State Health Facts for more details on each state’s private insurance law and Medicaid coverage, including contraceptive methods covered.)
For more information on how states have implemented insurance of OTC contraceptives, see KFF’s report Insurance Coverage of OTC Oral Contraceptives: Lessons from the Field and issue brief Over-the-Counter Oral Contraceptive Pills.
Pharmacist Prescribing
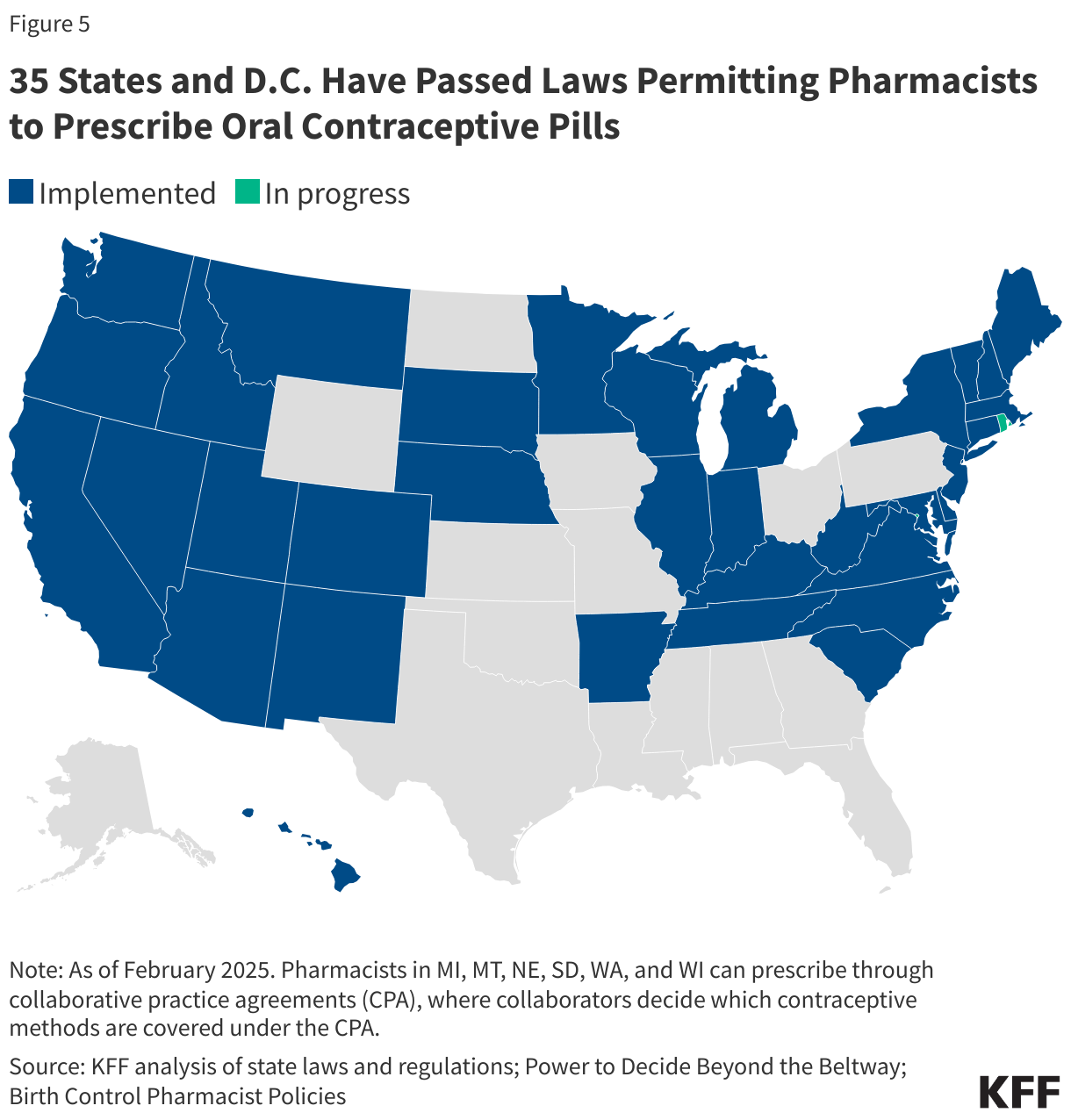
Another avenue that is gaining support in some states allows pharmacists to prescribe or dispense OCP without requiring an in-person medical visit to a physician. As of February 2026, 36 states and D.C. passed legislation to allow pharmacists to prescribe certain self-administered contraceptives to women (Figure 6). All of these states allow pharmacists to prescribe at least oral contraceptives, but states vary in other details, such as the type of prescriptive authority (e.g., collaborative practice agreements, statewide protocols, and standing orders), minimum age requirements, the type of contraceptive that pharmacists can prescribe, the length of the supply, and whether the patient needs a prior prescription from a physician.
Although expanded scope of pharmacist practice can remove some barriers to obtaining contraceptives, challenges still remain for women seeking a prescription for contraception from a pharmacist. For example, pharmacies typically charge consultation fees, which some reports suggest can be as high as $50 in certain areas. Although insurers are generally required to cover contraceptives without cost sharing, they are not obligated to cover this fee. Also, pharmacies can choose not to participate or may not have any pharmacists trained to provide this service.
From the pharmacy perspective, pharmacists must elect to complete additional education requirements, which vary by state, and often include several hours of continuing education from an accredited training program. Additionally, states may not have a reimbursement mechanism in place to pay pharmacists for providing this service. For example, while Oregon and Hawaii require plans to reimburse the dispensing entities, California’s law does not require reimbursement for payers other than Medicaid. Lack of or low reimbursement for pharmacist prescribing can result in fewer pharmacies choosing to provide this service.
12-Month Supply
Another approach to facilitate access to oral contraceptives involves increasing the dispensing period of contraceptives to 12 months per prescription. Currently, dispensing patterns vary by insurer, with many plans limiting supply of pills to 1-3 packs at a time. The 2022 KFF Women’s Health Survey found that among females who reported using birth control pills in the past year, 32% receive 1-2 packs at a time, 63% receive 3-5 packs, and just 3% receive a 12-month supply. Providing women with an extended supply of pill packs may lead to more consistent contraceptive use. Women who receive a one-year supply have been found to be 30% less likely to have an unintended pregnancy compared to women receiving a 1–3-month supply.
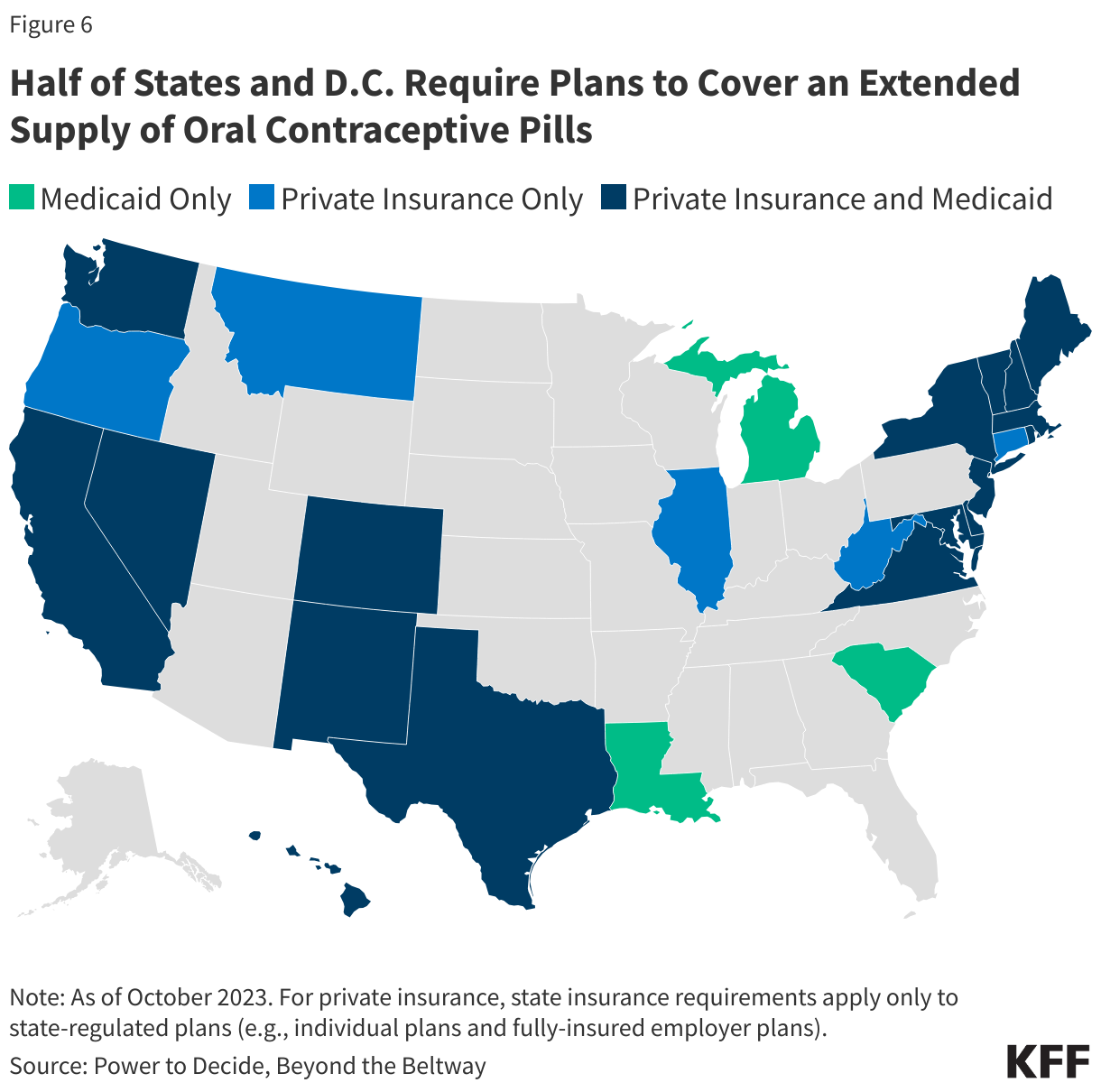
In 2015, Oregon became the first state to pass a law requiring state-regulated plans to cover a three-month supply of contraceptives when first prescribed, followed by a 12-month supply of contraceptives. Laws requiring coverage for 12 months of oral contraceptives have since been enacted in 29 additional states and DC (Figure 6). Idaho, Louisiana, and New Mexico require coverage for a 6-month supply. While most of these states have also enacted policies that require no-cost contraceptive coverage similar to the ACA’s contraceptive coverage provision, eight states (HI, ID, LA, MI, MT, OK, TX, and WV) with extended supply laws have not done so. This means that although insurers must cover a 12-month supply in these states, state law does not prohibit cost sharing; however, most plans must abide by the federal requirement and not charge any cost sharing for prescribed, FDA-approved contraceptive methods.
Telecontraception
In recent years, a growing number of companies providing contraception through online platforms (“telecontraception”) have entered the market and are providing a new option for people to obtain contraceptive supplies without the need for an in-person visit. A growing number of online services and smartphone applications offer options for patients to speak with providers by video or chat, get prescriptions, and order birth control pills through mail delivery. These services work by collaborating with physicians, pharmacies, and sometimes health insurers to prescribe and ship OCP to the patient’s home or a local pharmacy.
Costs for these services vary between companies. Most charge a fee for the service, which is typically not covered by insurance and can range from a $15 fee per consultation/prescription to a $99 yearly membership that covers the medical evaluation and customer support for the duration of the prescription.
A KFF study on telecontraception companies found considerable variation in method availability and acceptance of insurance. Many telecontraception companies accept private insurance and/or Medicaid, to pay for the cost of the pills, while others do not. The price of contraception offered by these platforms vary by method and by brand; generic pills typically range in price from $5 to $25 per pack without insurance.
Most companies ship OCPs free of charge to the patient’s home, while some require pick up from a local pharmacy. Prescriptions are often valid for 12 months and patients are sent either a one- or three-month supply of pills. Video/audio consultations are required by certain services before receiving the prescription. Services that do not require a consultation do require patients to complete a health assessment or questionnaire to determine eligibility and the appropriate pill. People in every U.S. state have access to at least one of these services, but the minimum age to use the service varies by company and state law, although many require the person to be at least 18 years old.
Oral contraceptives are the most commonly used form of reversible contraception in the U.S. Most women with private insurance or Medicaid can receive no-cost coverage for OCPs. The FDA recently approved Opill, the first ever daily OCP available over the counter, though insurance coverage of the product will largely depend on state efforts in the absence of federal guidance.Several states have enacted policies to broaden OCP access, particularly through pharmacist prescribing and insurance coverage for extended supplies and non-prescribed OTC contraceptives. The use of telemedicine to expand OCP access continues to evolve, with many women now able to obtain OCP using smartphone and web-based services.