

Worsening fiscal constraints and changing policy priorities have resulted in significant funding cuts to global health and development programs. While these reductions predated the cuts and disruptions made by the U.S. government last year, they were exacerbated by U.S. actions. The Organisation for Economic Co-operation and Development (OECD) recently reported that international aid fell significantly in 2025, driven primarily by the U.S., and that further declines are likely on the horizon. The health sector has not been immune to these pressures. The U.S. government and the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), the top two donors1 to global health in low- and middle-income countries, each took actions to reduce funding to countries starting last year and plan to further reduce funding going forward. Under the Trump administration, the U.S., as part of its new America First Global Health Strategy (AFGHS) “MOU” agreements with countries, plans to reduce funding by billions over the next few years. The Global Fund, due to reduced contributions from the U.S. and other donors, is also reducing funding in the same set of countries. Together, the U.S. and Global Fund reductions serve as a “one-two punch” to countries, who will be faced with significantly fewer resources in the coming years.
This analysis assesses the magnitude of these combined funding cuts in 29 U.S. MOU countries between 2026 and 2029, relative to prior funding levels (see methodology for more details). As it shows, the combined decline is estimated to total $4.3 billion– a 24% drop relative to prior funding levels — most of which (77%) is driven by the U.S. The cumulative cut, taking into account unexpected reductions in 2026, was even larger, reaching $5.8 billion. Moreover, further declines are likely to occur after this period.2 Such funding declines are unprecedented in the modern-day era of global health, which saw the creation of the President’s Emergency Plan for AIDS Relief (PEPFAR), the U.S. government’s flagship global health program, and of the Global Fund in the early 2000s, both of which helped to usher in significant new resources for global health.
Findings
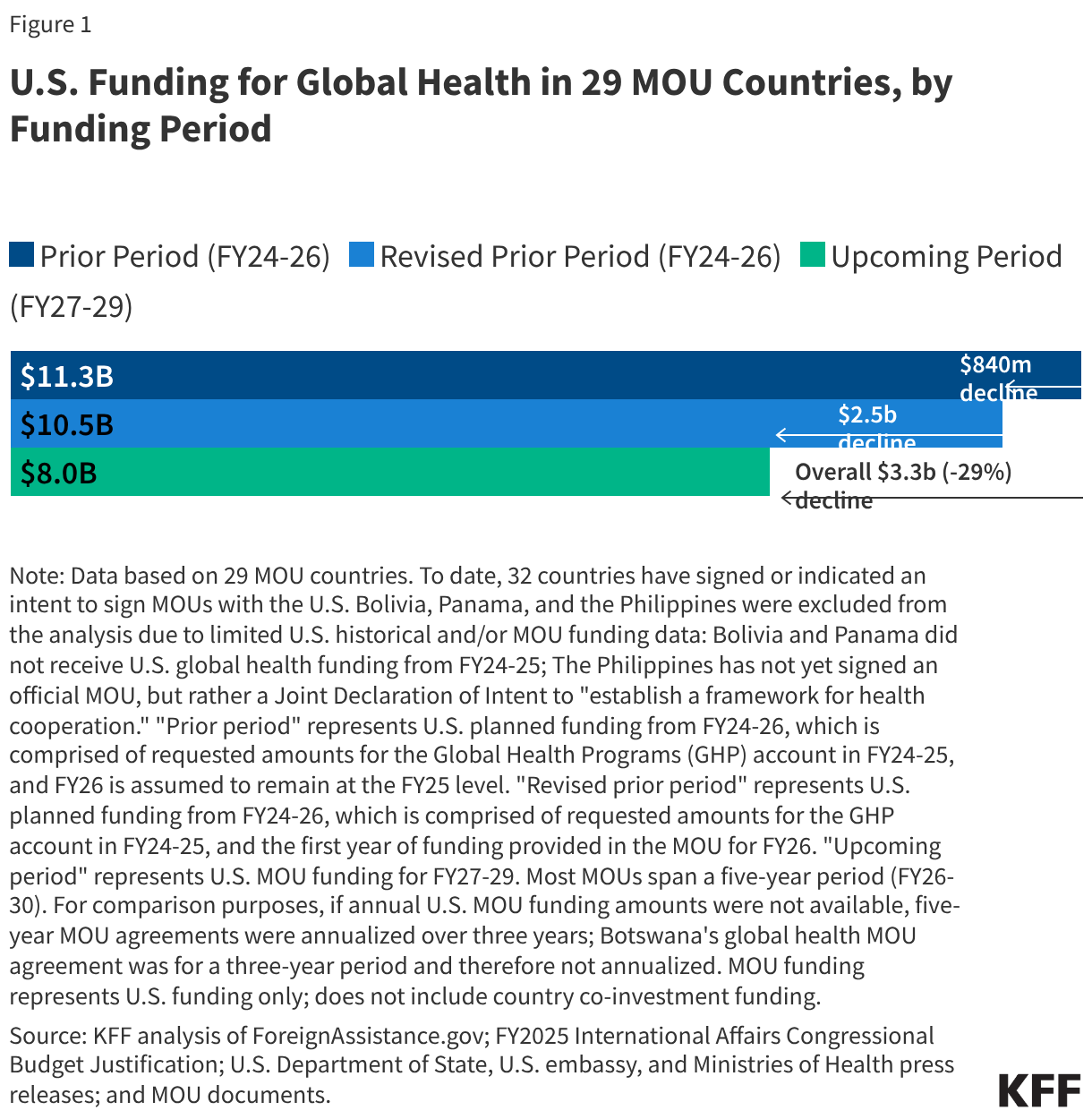
The U.S. government is planning steep funding cuts to countries for health programs. In the 29 MOU countries analyzed, these cuts are estimated to total $3.3 billion by 2029, a 29% drop relative to prior funding levels.
- Overall, funding in these 29 countries is estimated to decline from $11.3 billion over the prior three-year period (2024-2026) to $8 billion for the next three-year period (2027-2029), a 29% decline. This decline reflects two factors: first, after several years of stable funding for countries, the administration announced significant reductions starting in 2026, relative to prior levels, estimated to be $840 million, or 7%; second, further reductions of $2.5 billion or 23% are planned for 2027-2029 (see Figure 1).
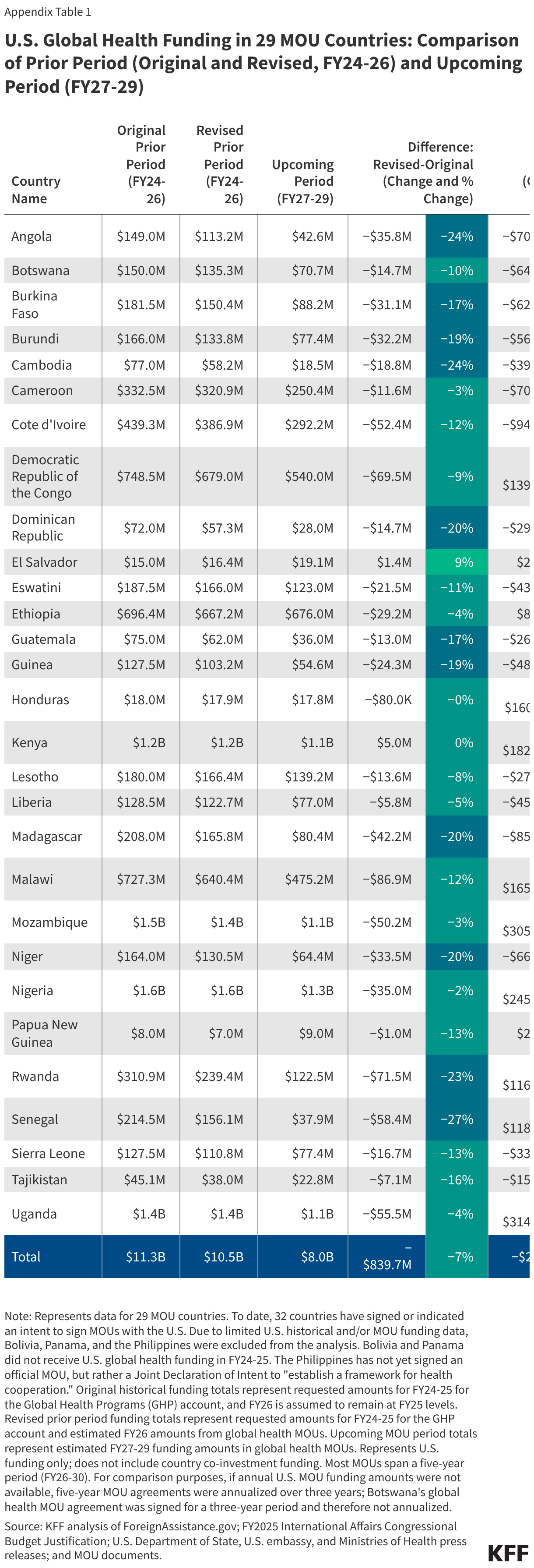
- Almost all 29 countries will face funding reductions.3 The countries with the biggest reductions in dollar terms are Uganda ($370 million), Mozambique ($356 million), Nigeria ($280 million), and Malawi ($252 million). Reductions range from 1% in Honduras to 82% in Senegal, with 12 countries experiencing reductions of 50% or greater (see Appendix Table 1).
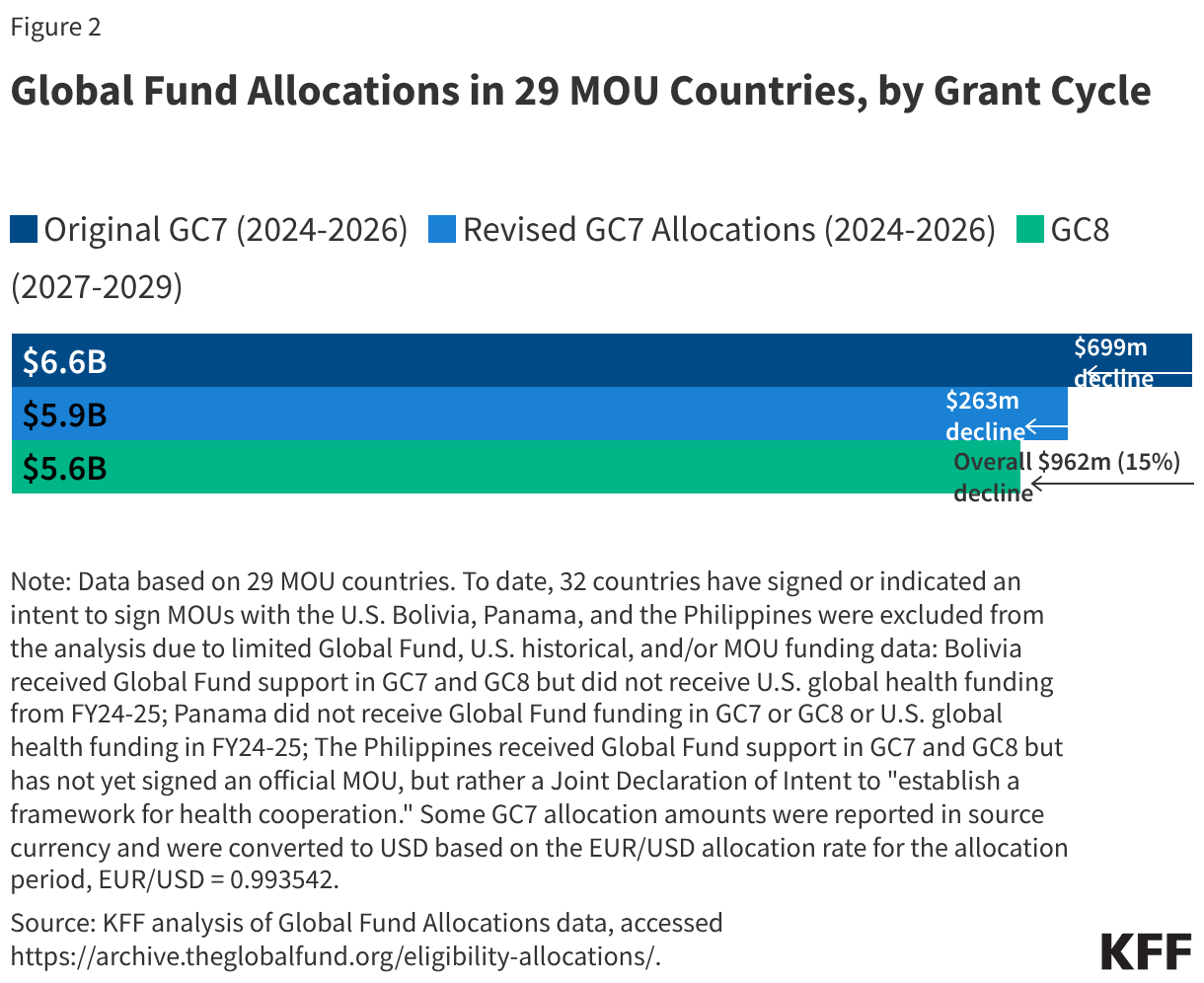
In these same 29 countries, Global Fund support is expected to decline by almost $1 billion over the next three years, a 15% drop compared to the prior period.4
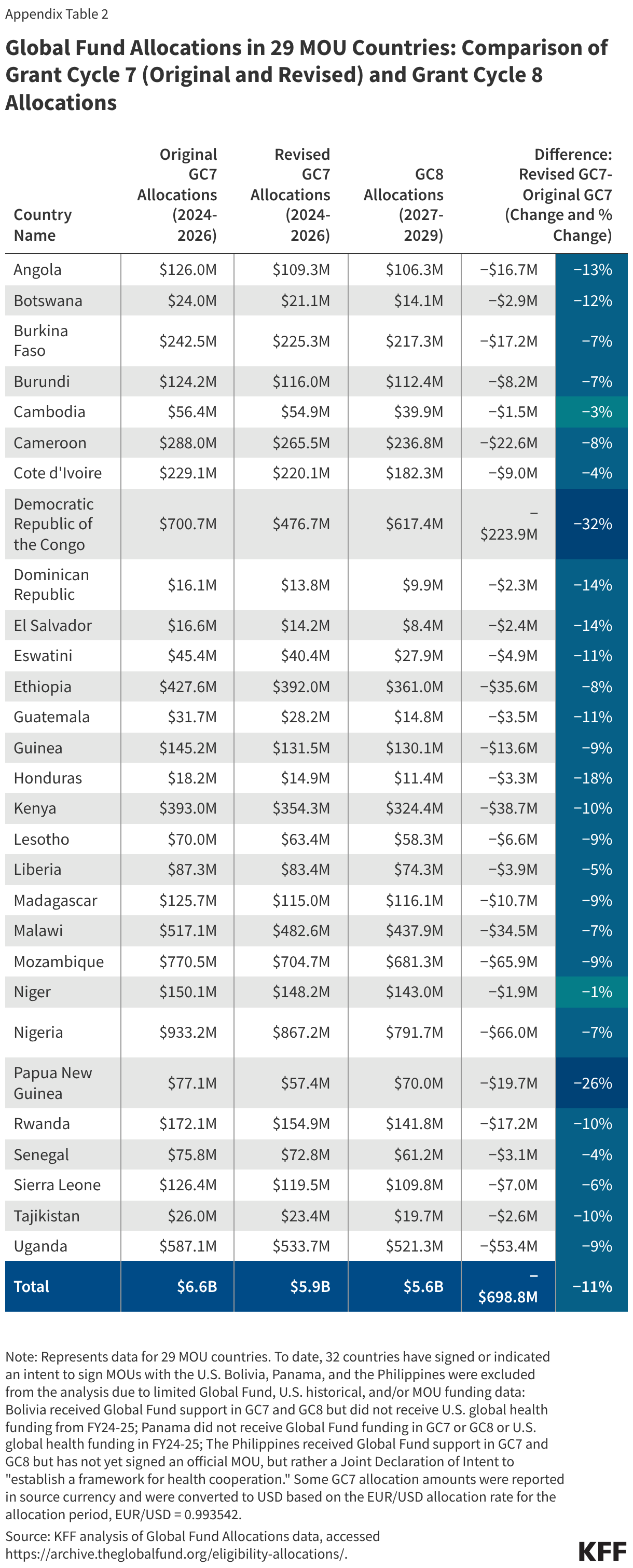
- Global Fund support will decline from $6.6 billion in the 2024-2026 country allocation period (grant cycle 7, or GC7) to $5.6 billion in the 2027-2029 allocation period (grant cycle 8, or GC8), a decline of $962 million or 15%. This decline is the result of the following two factors: a reduction in the original funding allocated to countries for GC7, due to unexpected shortfalls in donor contributions to the Global Fund (a reduction of $699 million or 11% from the original to revised allocations), and further reductions planned for GC8 due to ongoing funding constraints (a reduction of $263 million or 4% from revised GC7 allocations to GC8 allocations) (see Figure 2).
- All 29 MOU countries will face Global Fund reductions. The countries with the biggest dollar reductions in GC8 (compared to the original allocations for GC7) are Nigeria ($141 million), Mozambique ($89 million), and the Democratic Republic of the Congo ($83 million). Reductions range from 5% in Niger to 53% in Guatemala (see Appendix Table 2).
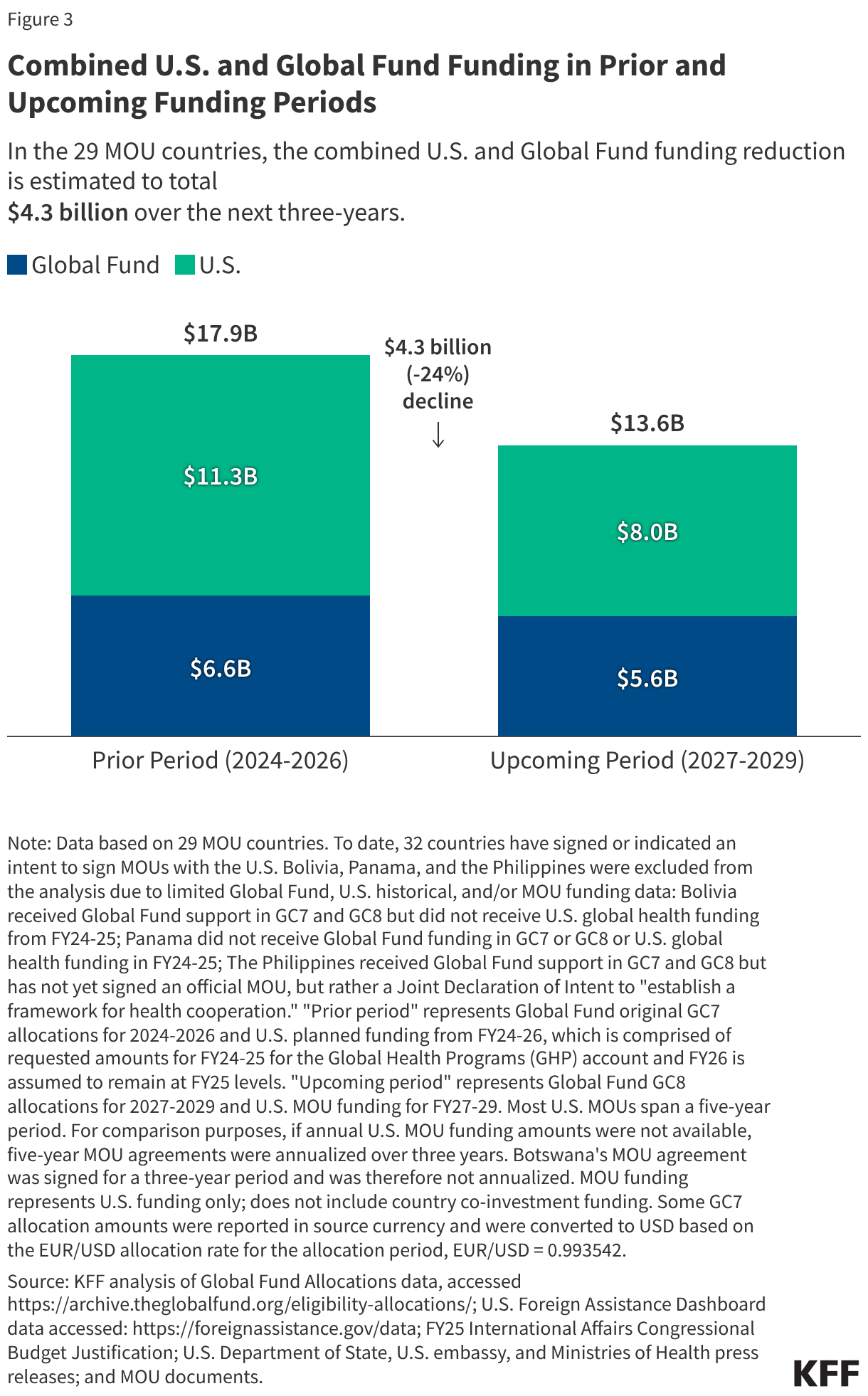
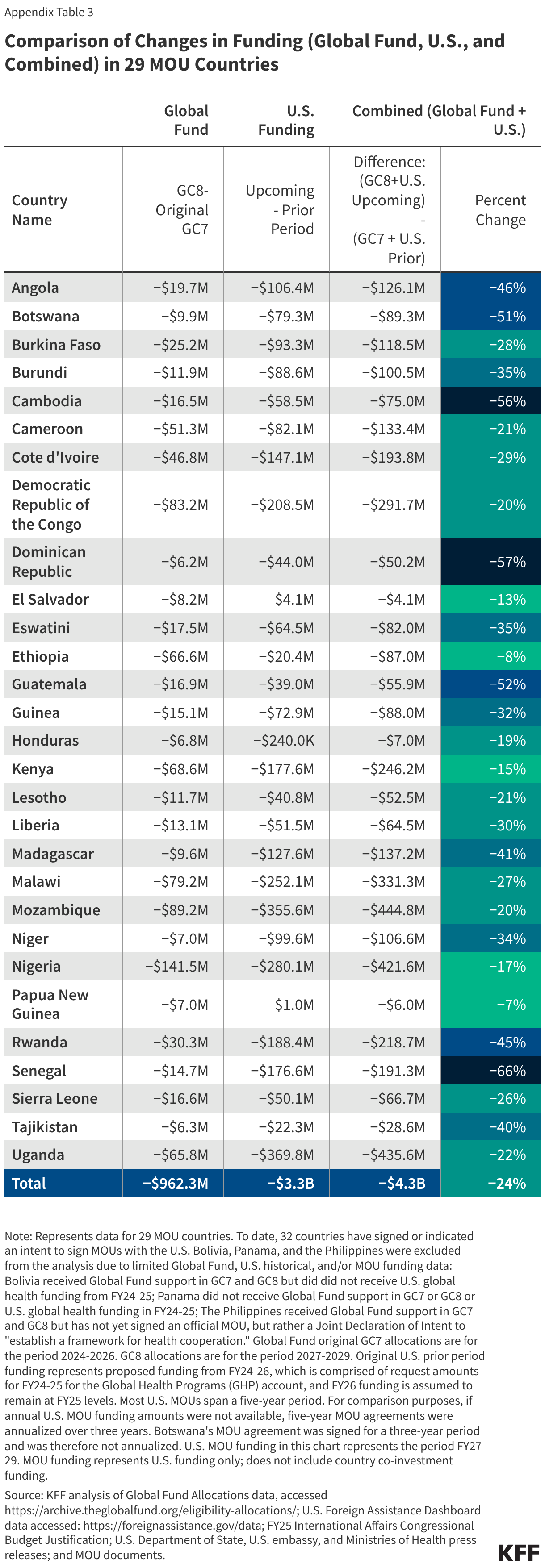
The combined funding reduction from the U.S. and the Global Fund in these 29 countries is estimated to total $4.3 billion through 2029, a 24% decline (see Figure 3). The U.S. accounts for more than three quarters (77%) of the drop.
- About half (15) of the MOU countries will experience funding reductions of $100 million or more, with the largest reductions in Mozambique ($445 million), Uganda ($436 million), Nigeria ($422 million), and Malawi ($331 million). Reductions range from 7% in Papua New Guinea to 66% in Senegal (see Appendix Table 3). The cumulative cut, taking into account unexpected reductions in 2026, was even larger, reaching $5.8 billion.
- In addition to these funding reductions, these countries also face co-financing requirements from both the U.S. and the Global Fund – with the U.S. requirement occurring for the first time – which could, in some cases, intensify the fiscal impact on recipient countries while offsetting some of the effect of the reductions on global health programs.
Looking beyond 2029, further declines are expected from the U.S., with an uncertain forecast from the Global Fund, as other donor governments are scaling back.
- The U.S. government plans to scale back funding in these 29 countries by an additional $2 billion in 2030 as it seeks to move programs to country governments (the full cut planned for 2027-2030 is estimated to be $5.3 billion).
- While the funding envelope for the Global Fund’s next grant cycle (GC9) is not yet known,5 the fiscal environment suggests additional reductions may lie ahead. In addition, five of the 29 MOU countries will transition out of Global Fund eligibility for at least one disease (HIV, TB, or malaria) by the next grant cycle: Botswana, the Dominican Republic, El Salvador, Guatemala, and Honduras.6
- More broadly, other donor governments (that provide direct aid to countries as well as support for the Global Fund) have also been scaling back their health and development assistance.
Funding declines of this magnitude are unprecedented in the modern-day era of global health, which saw the creation of the Global Fund in 2002 and the launch of PEPFAR in 2003, both of which helped to usher in significant new resources for global health.
- As such, this next period will mark a significant departure in the global health response, with countries expected to move increasingly away from dependency on external support for health, while simultaneously ramping up their own expenditures. This will likely pose challenges for at least some of these countries, particularly those facing significant co-financing requirements and experiencing or at risk of debt distress and/or fragility or conflict, and will impact the millions of people whose health has benefited from these efforts.
Appendix
Methodology
To assess the impact of funding changes on countries that receive U.S. and Global Fund funding for global health activities, we analyzed funding in three ways. For the 29 countries with signed MOUs and available data, we compared 1.) U.S. MOU funding to historical U.S. planned and proposed funding amounts, 2.) the Global Fund Grant Cycle 8 (GC8) allocations to Grant Cycle 7 (GC7) allocations (both original and reduced GC7 amounts), and 3.) the combined impact of funding changes to U.S. and Global Fund funding. U.S. planned/proposed funding amounts were obtained from ForeignAssistance.gov for FY24, the FY2025 International Affairs Budget Request for FY25 (and FY26 original amounts), and MOU agreements for FY26 revised amounts. U.S. MOU funding amounts were obtained from U.S. Department of State, U.S. embassy, and Ministries of Health press releases, as well as MOU documents if available. Global Fund allocations were obtained from the Global Fund’s ‘Eligibility, Allocations & Funding’ data: https://archive.theglobalfund.org/eligibility-allocations/.
U.S. Funding Comparison: In countries that have signed bilateral global health agreements with the U.S., we compared U.S. MOU funding to what countries had historically received from the U.S. for global health in prior years. “Original prior period” funding represents FY24-FY26 funding; FY24-FY25 represent requested amounts and FY26 was assumed to remain at the FY25 level. “Revised prior period” funding represents FY24-FY26 funding; FY24-FY25 represent requested amounts and FY26 represent the first year of funding (FY26) provided in the MOUs. Most signed MOUs span a five-year period (FY26-FY30). To match the Global Fund’s three-year grant cycle period, if annual funding amounts were not available, five-year funding was adjusted to estimate a three-year total (for FY27-FY29) and compared to the prior three-years of U.S. proposed funding (FY24-FY26). For countries whose annual MOU amounts are not yet available (all but eight), MOU funding amounts were calculated to be spread evenly throughout the five-year period. Based on the eight MOU countries whose annual funding amounts were available (Cameroon, Ethiopia, Kenya, Liberia, Mozambique, Nigeria, Rwanda, and Uganda, which together account for 70% of U.S. MOU funding over the five-year period), the U.S. provides more funding to countries in earlier years of the MOU agreement, with steeper cuts occurring at the end of the five-year MOU period. While 32 countries to date have signed or indicated an intent to sign MOUs with the U.S., for comparison purposes, this analysis is based on 29 countries, as three (Bolivia, Panama, and the Philippines) have limited data on Global Fund allocations, U.S. historical, and/or planned MOU funding (Bolivia received Global Fund support in GC7 and GC8 but did not receive U.S. funding for global health in FY24-FY25; Panama did not receive Global Fund support in GC7 or GC8 and did not receive U.S. funding for global health in FY24-FY25; and the Philippines received Global Fund support in GC7 and GC8 but did not sign an official MOU but rather a declaration of intent to “establish a framework for health cooperation”).
Global Fund Comparison: In the same set of 29 countries, we compared GC8 allocations to GC7 (both original and reduced) allocations. The GC7 replenishment period was 2023-2025 with the country implementation/allocation period spanning 2024-2026; The GC8 replenishment period is 2026-2028, with the country implementation/allocation period spanning 2027-2029. Some GC7 allocation amounts were reported in source currency and were converted to USD based on the EUR/USD allocation rate for the allocation period, EUR/USD = 0.993542.
Combined Funding (Global Fund + U.S.) Comparison: To assess the combined impact of Global Fund and U.S. funding changes in MOU countries, we compared the sum of the original GC7 allocations and U.S. historical global health funding over the same period (FY24- FY26) with the sum of the GC8 allocations and U.S. MOU funding for the following period (FY27-FY29). If annual U.S. MOU amounts were not available, three-year adjusted totals were used.
Jen Kates currently serves on the board of the Global Fund to Fight AIDS, Tuberculosis and Malaria.